Abstract
Background
Antibody-mediated immune response plays an important role in protection against reinfection. In the case of SARS-CoV-2 infection, the maximum duration of antibody response is still unknown. In this work, the generation of neutralizing antibodies (NAbs) and IgG antibodies against the S1 subunit (S1 IgG ) of SARS-CoV-2 and their possible duration were determined through decay models.
Methods
132 participants with SARS-CoV-2 infection were classified according to the severity of the disease. Seroconversion and persistence of S1 IgG antibodies and NAbs were determined by ELISA, samples were taken at two different times post-infection and duration of those antibodies was estimated using Linear Mixed Models (LMMs).
Results
The highest amount of S1 IgGs antibodies was associated with age (41 years or older), greater severity of COVID-19 and male gender. NAbs production was associated with the same variables, except for age. The percentage of NAbs decay is higher in the asymptomatic group (P = 0.033), while in S1 IgG antibodies decay, no statistical difference was found between the 4 severity groups. An exponential decay model was built by using a LMM and similarly, two dispersion regions where constructed. The duration of S1 IgG antibodies was 744 days (668–781) for first region and 744 days (453–1231) for the second. Regarding NAbs, an adaptative LMM was used to model a logistic function, determining a duration of 267 days (215–347).
Conclusion
Humoral immunity to SARS-CoV-2 infection depends on the severity of the disease, gender and age. This immune response could be long-lasting as for other coronaviruses.
Introduction
Infection with the Severe Acute Respiratory Syndrome virus 2 (SARS-CoV-2) could be asymptomatic or generate the disease called COVID-19, with a wide clinical spectrum [1]. The humoral response against SARS-CoV-2 has been described in detail in the convalescent phase [2], however, its duration is not yet fully known. The structural protein spike (S) of SARS-CoV-2 is an important target for the production of antibodies and is divided into two subunits: S1 and S2 [3]. The S1 subunit contains the receptor-binding domain (RBD), and it’s through this domain that the spike protein recognizes and binds to its receptor on the target cell, angiotensin-converting enzyme 2 (ACE2) [4]. The S2 subunit mediates the fusion between the viral and the cell membranes [5]. Antibodies against RBD region could block key interaction sites between SARS-CoV-2 and ACE2, preventing the virus from entering the cell [6], hence they are known as neutralizing antibodies (NAb). Antibodies directed against RBD region represent up to 90% of the neutralizing activity in sera from patients infected with SARS-CoV-2 [7]. NAbs have been found against other regions in the S1 [8] and S2 subunits, the same has been reported for other coronaviruses such as the Severe Acute Respiratory Syndrome virus (SARS-CoV) and the Middle East Respiratory Syndrome virus (MERS-CoV) [9].
The generation of IgG antibodies against the S1 subunit (S1 IgG) of SARS-CoV-2, reaches its maximum peak at 21–49 days post-symptoms start, while the NAbs reach their maximum level at 14–22 days, gradually decreasing through the time [2]. Most recent data indicate that S1 IgG and NAbs antibodies against SARS-CoV-2 could last up to 270 days [10] depending on the severity of the infection [11]. The maximum duration of NAbs and S1 IgG antibodies is still unknown. In this study, the aim was to determine the production of NAbs and S1 IgG antibodies, as well as their possible duration using prediction models, in a human population that includes asymptomatic with SARS-CoV-2 infection and patients with different clinical manifestations of COVID-19.
Methods
Study design and participants
A longitudinal and exploratory study was developed. The inclusion criteria were to be older than 18 years, to be positive for SARS-CoV-2 by RT-qPCR with at least 27 days post-infection. Since there are participants with and without symptoms, we use the term post-infection for both groups. In the case of symptomatic patients, it refers to the date of symptoms onset whereas for asymptomatic patients refers to date of contact with a confirmed case of COVID-19. Eight participants with a positive result by serology were included. These last participants were cohabitants of positive cases by RT-qPCR. The serological test (Edinburgh Genetics Limited) was approved by the Mexican authorities was used [12].
Recruitment was made from August 26 to November 23, 2020, at the Centro de Alta Especialidad “Dr. Rafael Lucio” (CAE) in the city of Xalapa and at Sanitary Jurisdiction No. VII of the city of Orizaba, Veracruz, México. After signing the informed consent, 132 participants were included and two peripheral blood samples were taken at two different days post-infection to obtain serum, which were stored at − 80 °C until analysis. A third sample was taken from three participants with different clinical manifestations. The sample of two participants, one mild and the other moderate, was taken at 183 days post-infection whereas the sample of the third participant, a severe case, was taken at 220 days post-infection.
Variables
Clinical and sociodemographic variables were collected through a face-to-face interview using an instrument developed and piloted by the authors. The classification of the severity of the SARS-CoV-2 infection in 4 groups (asymptomatic, mild, moderate and severe) was carried out based on the ordinal scale of eight categories of the National Institutes of Health (NIH) [13, 14].
S1 IgG antibodies detection
An ELISA kit was used for the detection of S1 IgG against SARS-CoV-2. The samples were processed and analyzed according to the manufacturer’s specifications (#2606–9620 G, EUROIMMUN). The results were expressed semi-quantitatively by the index, dividing the value of the optical density (O.D.) of each serum (average of the duplicate) by the value of O.D. of the calibrator. Values ≥ 1.1 are considered positive.
Competitive ELISA
A surrogate viral neutralization test was designed through a competitive immunoassay that detects NAbs that block the S-ACE2 protein interaction, as has been reported [15, 16]. Briefly, 96 well plate was sensitized with 2 µg/ml of ACE2 protein (20 h at 4 °C, #10,108-H08B, Sino Biologicals). Then was blocked with BSA 1% PBS for 1 h at 37 °C. Serum samples were diluted 1:10 in PBS 1x (in duplicate) and incubated 1 h at 37 °C with recombinant Spike protein (final concentration 2 µg/ml, obtained from BEI Resources, NIAID, NR-53257). This mixture was added to a previously sensitized and blocked 96 well plated and incubated for 1 h at 37 °C. Subsequently, the secondary antibody IgG-HRP (#7074, Cell Signaling Technology) diluted 1:3000 was added in PBS/Tween 0.1%, BSA 0.01% for 1 h at 37 °C, followed by 30 min with the substrate HRP (#P9187, Sigma Aldrich) incubated at the same temperature. Finally, the stop solution (HCl 3 M) was added. Three washings steps with PBS/Tween 0.1%. were performed between each incubation. The samples were read at 493 nm. The results are shown as a percentage of the neutralization calculated based on the following formula:
where 0.071 corresponds to the signal obtained when incubating the primary antibody rabbit anti-S SARS-CoV-2 (#40,592-R001, Sino Biologicals) and secondary independently. A cut-off point was established using the mean of values obtained with pre-COVID-19 sera.
Decay models
Exponential decay model
The S1 IgG antibodies decay was modeled by an exponential function (Eq. 1) which parameters were obtained by a linear mixed model (LMM).
Central model curve was obtained by fitting an exponential curve to each individual and then selecting parameters as the median of the group. Two interval regions where computed: one considering only variations at the origin of the curve (i.e., modifying only the parameter a in Eq. 1), and the second interval region, considering both variants (i.e., parameters a and b, in same equation). Variants consider the quartiles one and three of mentioned parameters.
| a (Q1, Q3) | b (Q1, Q3) |
|---|---|
| 9.33904 (7.50534,10.38107) | − 0.00288 (− 0.00424, − 0.00182) |
Then following crossing (solutions) where found:
| Model 1 Days (Min, Max) |
Model 2 Days (Min, Max) |
|---|---|
| 744 (668,781) | 744 (453, 1231) |
Logarithmic decay model
Differently from previous model, but based on the behavior of data, NAbs decay was modeled as a negative sigmoid or logistic function as described by Eq. 2.
where θ1, θ2 and θ3 represent the maximum size, decay rate and lag phase, respectively. On this case, due to variability displayed in data, an adaptive LMM was used.
Considering NAbs represented as percentage then θ1 = 100. The next two parameters were obtained by clustering data as follows: a first group of individuals with decay rate inferior to 10% but with NAbs values above 90%. A second group with decay rates greater than 10% and the rest of individuals.
The second group is used to determine the decay rate of the group, while lag phase was determined by the first group. However, as number of individuals on each group is quite different, the decay rate model frontiers were obtained by quartiles one and three, however, for lag phase a minimal and maximal values where used.
| θ2 (Q1, Q3) | θ3 (Min, Max) |
|---|---|
| − 0.02390 (− 0.03620579, − 0.01534895) | 143 (133, 155) |
Crossing where obtained for the value of 5% of NAbs.
| Days (Min, Max) | |
|---|---|
| 267 (215, 347) |
Statistical analysis
The comparison of categorical variables (sociodemographic characteristics and comorbidities) was analyzed using the Chi-Square test; S1 IgG antibodies and NAbs indices and percentages of decrease did not comply with the assumption of normality, therefore, when they were compared by the level of severity and days post-infection the Kruskall-Wallis test was used. When these same variables were compared by sex and age group, the U-Mann Whitney test was applied. The Wilcoxon test was used to compare the percentages of decrease in the S1 IgG index and NAbs between the first and second sampling. The level of statistical significance was considered when p value was less than 0.05. For the statistical processing of the information the SPSS statistical package was used (IBM SPSS Statistics 21.0; SPSS Inc.).
Results
Study population
132 participants were included, 13.6% were asymptomatic, 48.5% mild, 26.5% moderate and 11.4% severe. 55.3% (73/132) were women and 44.7% (59/132) men. 61% (36/59) of the men had moderate or severe COVID-19 and 80.8% (59/73) of the women had mild or asymptomatic SARS-CoV-2 infection (P ≤ 0.001). Patients with diabetes and cardiovascular diseases developed more severe symptoms of COVID-19 (P = 0.030 and P = 0.046, respectively) (Table 1). The median of first and second sampling were carried out, respectively, at 72 (66–75) and 138 (132–150) days post-infection for the asymptomatic group; 63 (51–84) and 141 (132–162) days for the mild group; 78 (66–90) and 153 (141—165) days for the moderate group and 72 (45–90) and 135 (126–156) days for the severe group.
Detection of S1 IgG antibodies against SARS-CoV-2
S1 IgG antibodies against SARS-CoV-2 were determined in the two samples from each participant by ELISA. 4.54% were seronegative in the first sample and 3.78% in the second, because an asymptomatic case seroconverted in the second sample. A third sample was taken from three participants, all of them had detectable antibodies. All seronegative participants were SARS-CoV-2 positive by RT-qPCR.
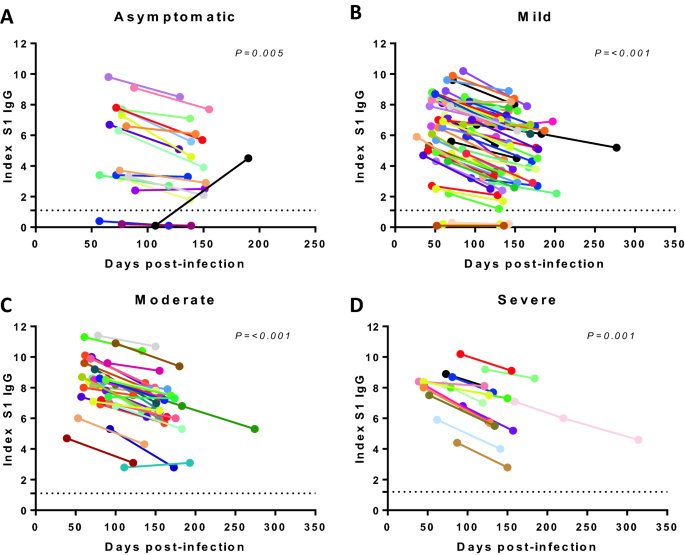
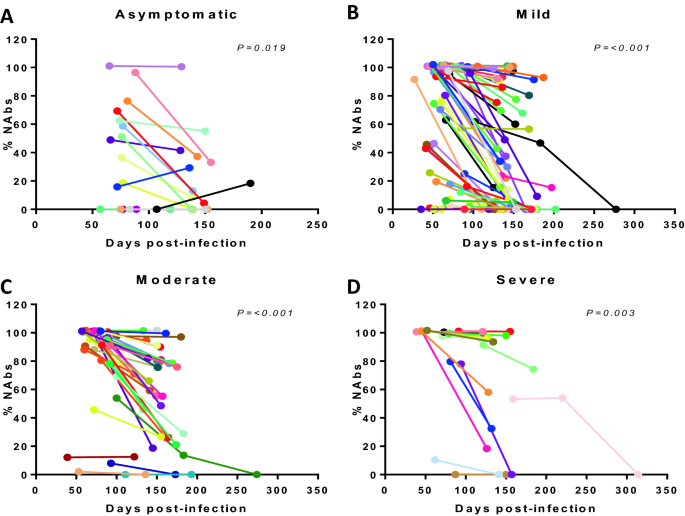
It was found that the S1 IgG indices increase with severity in both samplings, with higher values in the moderate and severe group (P ≤ 0.001) (Tables 2 and S1). The decay of S1 IgG between the first and second sampling was expressed as a percentage (Fig. 1), It was found that the decay is faster in the asymptomatic group (median 21.49%) without finding any statistical difference between the severity groups (Table 2).
The analysis by sex of the S1 IgG antibodies indices shows that men had higher values in both samplings (P = 0.006 and P = 0.010, respectively). The median age was 41 years, and it was used as a criterion to divide the population into 2 groups. Participants 41 years of age or older showed higher rates in both samplings (P = 0.001 and P = 0.003, respectively). There were no significant differences in the decline of the indices by sex or age (Table 3).
Detection of NAbs against SARS-CoV-2
For the detection of NAbs a competitive ELISA was used, which quantifies the inhibition of the interaction between RBD and ACE2, expressed as a percentage. 89.7% of the participants positive to S1 IgG antibodies, presented NAbs in the first sample and 73.2% maintained detectable Nabs in the second sampling. The sera of the participants of the third sampling did not have neutralizing activity. The NAbs were higher as the severity of the infection increased, in the first (P ≤ 0.001) and second sampling (P = 0.001). The percentage of decay by severity group was determined, between the values of sampling one and two (Fig. 2), finding a statistical difference between the 4 groups. The decay was greater in the asymptomatic group (median 65.76%, P = 0.033) (Tables 2 and S1).
The analysis by sex revealed that men presented higher levels of NAbs in both samplings (P = 0.003 y P = 0.012, respectively). Regarding age, no statistical difference was found even though people over 41 years old showed higher levels of NAbs in the first sampling.. The decline by sex or age was not significant (Table 3).
Estimation of the duration of S1 IgG antibodies and NAbs using LMM
To estimate the duration of S1 IgG antibodies, an exponential decay model was proposed. The parameters were obtained using a LMM that includes all participants. Based on the indices and exponential decay of the antibodies from the first and second sampling, two variants of the interval region were obtained: one with changes only at the origin of the curve and the second one, at the origin and the slope. The variants suggest a mean duration of A) 744 days (668–781) and B) 744 days (453–1231) (Fig. 3A).
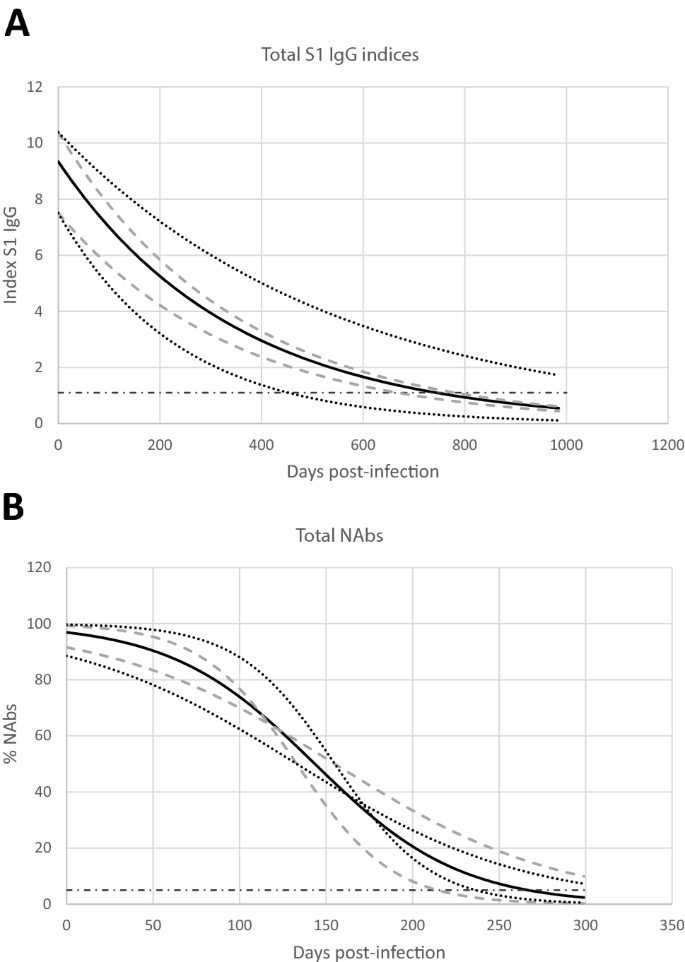
The S1 IgG antibodies results corresponding to the third sample of the 3 participants with the longest time post-infection by SARS-CoV-2 were used to verify the models. The results show a detection of S1 IgG antibodies in a severe case up to 314 days. The S1 IgG antibodies results of the three participants fall within the interval defined by the quartiles, of model B.
Similarly to the S1 IgG antibodies, the duration of NAbs was modeled as a negative sigmoid curve, model derived from the behavior of the data. On this case, as it has been explained previously, an adaptive LMM was used. The models show that the NAbs have a duration of 267 days (215–347). In the third sampling, no neutralizing activity was detected, which is consistent with the proposed model.
Discussion
Antibody mediated immunity represents one of the most important mechanism in protection against viral infections [17], in the case of SARS-CoV-2 is not yet fully known. This subject of study has been of great interest without excluding cellular immunity, whose role in the protection of reinfection has been highlighted lately [18].
One of the aims of this work was to address the production of IgG antibodies against the S1 subunit, which generate the highest amount of NAbs because it contains the RBD region. We found that 4.54% of the participants did not seroconvert to S1 IgG antibodies against SARS-CoV-2. This could be due to the fact that a short-term antibody response was induced or these were not produced, as has already been reported for an asymptomatic or mild infections by SARS-CoV-2 [19,20,21]. Monitoring and studying the reasons for this seronegative group is extremely important. There is evidence that this population has a delay in the control of viral infection and they have an increased risk of death in these individuals [22]. In this work, it was not evaluated whether seronegative individuals generated cellular immunity against SARS-CoV-2.
Initial reports suggested that IgG antibodies against SARS-CoV-2 could be short-lived, around 3 months [23, 24], leaving the possibility of reinfection after that period. In this work we detect S1 IgG antibodies up to 147 days post-infection on average, in all participants of the second sample and up to 314 days in a severe case of COVID-19 of the third sample, which suggest a longer persistence than reported and that it is similar to that observed for human seasonal coronaviruses [25]. Due to the recent circulation of SARS-CoV-2 and the prompt application of the vaccine, the maximum duration of IgGs due to natural infection may not be known. Based on the above, mathematical models are an important tool in estimating the duration of IgG antibodies and have been used in some studies for SARS-CoV-2 [26, 27]. In this work, based on LMM models, the maximum duration of S1 IgG antibodies was 744 days for the studied population, which suggests an adequate and similar immune response for other viruses such as SARS-CoV and MERS-CoV [28].
The detection of NAbs is essential, since they are the antibodies that prevent the virus from entering its host cell [29]. In SARS-CoV-2 infection, the NAbs correspond to a cocktail of antibodies, the majority directed to the RBD region [7]. In this work, the presence of the NAbs found in the S1 subunit containing the RBD region was determined by a surrogate virus neutralization test through a competitive ELISA. The results show that 85.07% of the participants presented detectable NAbs with our technique. The maximum duration of NAbs reported is 270 days [10]. In this work, we find NAbs up to 220 days, while the LMM estimated a maximum duration of 267 days. The determination of NAbs and the LMM model in our work allows us to generate important knowledge. We used a surrogate virus neutralization test based on antibody-mediated blockage of ACE2-S protein interaction to detect NAbs. Further studies involving SARS-CoV-2 pseudotyped lentivirus or the entire virus should be carried out; these are ideal techniques for the detection of NAbs [30]. Recently, it has been reported in neutralization assays using SARS-CoV-2 virus that NAbs titer has been correlated with protection against re-infection [31]. In this work, our LMM model fitted the behavior of NAbs in persons with different clinical manifestations of COVID-19 so it could be used as an individual predictor tool. The models to estimate maximum individual antibody duration could be relevant since recent reports suggest that NAbs longevity could be influenced by the time when maximum peak occurs as well as the decay rate [32]. It is important to highlight that in vitro test generate valuable information, however, in vivo the phenomenon of accelerated generation of antibodies occurs due to a second exposure to the pathogen [33,34,35]. This phenomenon has not been evaluated for reinfections by SARS-CoV-2, however, people who presented the natural infection added to an artificial immunization by vaccination [36, 37], presented a high generation of antibodies, which could favor a greater duration of IgG antibodies. Even greater reactogenicity has been reported in those individuals who were infected by SARS-CoV-2 and who received a second dose of vaccine [38]. One of the most important variables that could influence the generation and duration of S1 IgG antibodies and NAb a, is the severity of the SARS-CoV-2 infection [11]. In this work, the results show that the higher generation of S1 IgG and NAbs are associated with greater severity of COVID-19. The relative late generation of IgGs and NAbs [39] and the ratio of higher amounts of antibodies in people with severe COVID-19, suggests that these antibodies may participate in seroprotection rather than resolution of the disease. The foregoing is also consistent with our results on the percentage of decline in NAbs, which is lower with greater severity of COVID-19. It should be studied whether people who had moderate or severe COVID-19 have less probability of reinfection and less symptoms, in case of reinfection. An important aspect to consider about NAbs in the protection against re-infection is their neutralizing capacity against new variants of SARS-CoV-2. It has been reported a considerable reduction in the neutralizing activity against the variants of concern (VOC) in sera from infected patients during the first wave of the pandemic [40].In Mexico the SARS-CoV-2 lineages circulating when the study was performed were 20B/S:732A and 21C (Epsilon), the latter been reported towards the end of the work [41]. The possibilities of re-infection of these participants could be due not only to the decrease in the level of NAbs but also to the reduction of their effectiveness compared to the current circulating VOCs.
Consistent with other studies, men experienced more severe forms of COVID-19 [42, 43], as well as higher levels of S1 IgG antibodies and NAbs compared to women. A possible explanation could be at the level of immune response or hormonal influence, as has already been reported [44].
The results of this work suggest an adequate humoral immune response due to SARS-CoV-2 infection, which is related to variables such as the severity of the infection, sex and age. The seroprotection obtained by natural infection should be evaluated. However, given the application of emergency vaccines, this could not be done, hence the models for estimating the duration of antibody response are an important tool. Our models suggest a persistence of S1 IgG and NAbs, which should be considered in vaccination plans.
[“source=link.springer”]